The NHS Consultation, part 3: Your ideas for change
The Labour Government has launched a consultation on the NHS.
This is the third of three blogs documenting my responses to this consultation.
My ideas are as follows, structured in line with the consultation requirements.
Organise the NHS as a franchise, not a charitable trust dishing out money to whoever asks for it
The current structure of the NHS is rooted in the first half of the twentieth century, and in turn from Victorian days, when individual hospitals were built in towns with funding obtained from various wealthy benefactors. Each hospital was an independent entity, there was no coordinated service.This is largely still how it works, except the ‘wealthy benefactor’ is the government. Government is funding many hospitals and other projects up and down the country, without seeing them to be properly structured or co-ordinated, i.e. that the funding is put to the best possible use. The NHS should be more of a franchised organisation, like a network of motor dealerships, than a collection of independent businesses that do not work together, as is the case today.
For instance, the NHS funds MRI scanners at many hospitals. Patients attend more than one hospital; but practitioners can only see scans at their hospital - they cannot see the full information that the NHS has funded for any given patient. Hospital and Primary Care computer systems do not connect to each other. There are a multitude of trusts, each re-inventing the wheel every time something needs doing (for instance, producing a document on how to cope with a new oesophageal stent: a Google search on these keywords returns documents from North Tees and Hartlepool NHS Foundation Trust, Royal United Hospitals Bath, Chelsea and Westminster NHS Hospitals Trust and at least a further dozen NHS trusts, all for something that is the same irrespective of the trust you happen to have been treated in!).
This needs to change. There needs to be ONE set of computer systems to support the whole taxpayer funded NHS, that share data, and allow practitioners and patients to see all the information about a given patient. There needs to be ONE set of processes, and ONE set of supporting documentation for patients, the NHS cannot afford to be paying people to write the same document in Bath (and elsewhere) that someone in Hartlepool has already written. There needs to be ONE appointment system for the WHOLE NHS, managed by ONE contact centre, that runs 24 x 7 (like a bank’s contact centre - perhaps using offshore resources), so that patients can easily get through to someone who can change their appointments; having staff in a multitude of places managing appointments, often not working outside office hours, provides a poor service to patients and also to the NHS as a whole.
In short, it should not matter which hospital one is treated at, the treatment should be the same, the patient experience the same.
One benefit of this approach is that every NHS unit could be assessed for ISO9001 compliance to procedures, and the associated reports published.
This affects all aspects of the NHS.
It will take a long time to deliver - it is a long term change. It will also require much courage and determination to drive through, but is essential.
2 . Include the ‘Savoy Test’ as part of regular staff training
At the Savoy Hotel in London staff occasionally stay overnight, as a customer, so that they experience the services provided by the hotel from the customer’s point of view, and see the point of many of the tasks they and their colleagues undertake as part of their routine work.
This approach should be adopted for ongoing staff training in the NHS. For instance, hospital managers and ward staff should be required to spend a (probably sleepless) night on a noisy ward, with the call button out of reach, using a pad and waiting for it to be changed, rather than visiting the toilet, and sampling the meals and the manner in which they are provided.
This would obviously affect hospitals, but could be rolled out to other parts of the NHS.
It could be implemented quickly - provided there is capacity on the wards and the necessary staff goodwill to support it.
3. Use NHS resources effectively
The NHS has a poor record in terms of use of resources. Whole hospitals lie almost silent in the evening and at weekends, when availability of appointments and tests is very limited. No business would invest huge sums in buildings and equipment for them to only be used in office hours. More needs to be done in the evening and at weekends - often times that suit patients. (Few GP surgeries offer evening or weekend appointments - WHY?)
Better use of technology - such as appointment systems - would enable patients to interact more easily with the NHS; a single point of contact for all NHS appointments would support cost reductions (reducing the need for staff in each office managing appointments, replacing them with a mixture of onshore and offshore contact centre workers).
Text and email communication with patients should be coherent and indicate how to obtain clarification; the use of hyperlinks within texts should be discouraged. (Not all phones that can process texts can process hyperlinks).
There should be no place for fax machines in the NHS; scanners are far more flexible.
NHS resources, and NHS time, should only be used for NHS activity; staff should be restricted from using personal phones during working hours, and any staff use of apps and websites associated with social media, games, dating, pornography, gambling etc. during work time should be a disciplinary offence.
Staff at hospitals should be encouraged to work a professional, flexible working day; that is, start when needed and stay at work until the job is done - being paid for a day’s work, not per hour, and with rest periods as required. Having some staff start early and others later would allow for office support to be available at hospitals for longer periods, perhaps 8am to 8pm, providing a better service to the patient. At present there is a ‘4.30 rush’ for the doors by office staff at our local hospital, even causing local traffic jams. NHS administrative staff are well paid and should not work a limited, fixed set of hours every day. By moving many staff to a more professional basis of engagement, productivity will improve - there will not be the incentive to ‘work slowly so that some can be saved for overtime’.
This will affect all aspects of the NHS.
It could be implemented in a couple of years but will probably be opposed by the unions.
4. Treat the patient as the customer
There should be moves to structure financial rewards to trusts and clinics so that they benefit from ‘repeat customers’ and get paid for what they actually do; they should not be paid just by headcount of registered patients. Having said this, financial incentives to overtreat patients - perhaps giving unnecessary vaccinations - must be avoided.
It should become normal to provide copies of all patient records, and test results, to the patient concerned as a matter of course. Many test results that are sent to GPs or specialists already contain the key details that a reasonably intelligent patient will understand; paying for a highly paid doctor to be part of the process, doing little more than reading test results to a patient, is a poor use of NHS funding.
Patients should be provided with an annual statement of their NHS use - summarising diagnoses, conditions, etc. - from their Summary Care Record, and invite them to report anything missing or incorrect. This will enable the SCR to develop into a much higher-quality source of data, from which clinicians can make useful judgements. (At present SCRs feature so many omissions and errors that they are of little value.)
Staff at all levels should be encouraged to treat patients, their carers and families with respect, and their knowledge - of their own health - must be valued by NHS staff. At present ‘zero tolerance’ notices feature widely on NHS premises; these are hardly respectful of patients, many of whom might be concerned, upset or distressed at the time of their presence in the unit. Staff should be better trained to understand the needs of patients, and, when an incident does occur, lessons should be learned so that improvements are made benefiting everyone. There are too many people in the UK now who avoid contact with the NHS because they feel the initial points of contact to be unpleasant and unhelpful.
Consent should be properly obtained by NHS staff before recording anything said by, or relating to, a patient, or any third party. The apparent practice of recording gossip or theories on patient records without the knowledge of those involved should cease.
When contacting patients by phone NHS staff should be polite and courteous, introduce themselves, and undertake proper ID checks of the person to whom they are speaking - it is possible that the patient may not have picked up the phone when they called, and may have a similar name to the person who did.
No-one who works in the NHS should get priority treatment or access to a practitioner on the grounds of them working for the NHS; they are just a customer, and no more important than all the other patients waiting to be seen.
Mistakes, of whatever seriousness, when they occur in an NHS funded unit, must be admitted, and steps taken as soon as possible to minimise the impact on the affected parties. A culture of ‘continuous improvement’ must be fostered, where lessons learned from mistakes are fed back into process reviews, and the chances of similar problems arising in future are reduced.
Doctors, and other practitioners, when asked for an opinion must not accept the views of another practitioner without question. This attitude allowed Dr. Harold Shipman to murder in excess of 250 people. When asked for an opinion, clinicians must review all available information (not just that provided by the requester), and possibly arrange for further tests or checks if necessary to make their own, independent, judgement.
This latter point is of particular importance with the possible introduction of ‘assisted dying’.
This will affect all aspects of the NHS.
It could be implemented in a couple of years but will probably be opposed by the unions.
5. What constitutes ‘good health’, and the objectives of the NHS, need to be defined
Without clearly defined objectives an organisation lacks purpose, and cannot be properly structured to deliver anything efficiently.
There do not seem to be objectives or hence any clear purpose for the NHS: it seems to be just there, to fund whatever one or more doctors say will help them treat or care for patients.
This needs to change - doctors are, it could be said, taking advantage of the generosity of the taxpayer. There needs to be an agreed definition of what constitutes ‘good health’, what the NHS will fund by way of treatment, and what it won’t, so that patients can, if appropriate, arrange insurance to cover for certain risks - for example, if it were decided that the NHS would not pay for treatment for injuries obtained participating in motor sport, a participant could obtain separate cover for this risk.
(An example of such a definition might be ‘The NHS is there to provide treatment and care to British Citizens to enable them to fully contribute to society and enjoy the quality of life that might be expected of someone of their age. It will fund treatment for illnesses such as …(and a list of conditions given)…, and for injuries sustained in day-to-day life, excluding at work (where treatment should be funded by employers), driving a motor vehicle (where it will be funded by insurance), or undertaking hazardous sports…. ’.).
Doctors' potential conflict of interests - in essence, that they get paid for treating someone - when recommending treatment must rule them out of assessing who gets NHS treatment.
For ‘societal conditions’ - non life-threatening, fashionable treatments, perhaps, such as plastic surgery, IVF, sex changes, or operations or medication for conditions that could be addressed by other means, such as obesity - it needs to be clear to all as to whether the NHS will fund treatment; again, the conflicts of interests in the medical industry should make this a non-medical decision.
Whatever the total scope of NHS funded treatment, it must be limited, and managed: there should be no opportunity for ‘scope creep’ as new ‘experts’ diagnose new conditions for which treatment requires funding.
As well as clinician conflicts of interest, the possible reasons for recommendations from supranational bodies - such as the WHO, significantly funded by the Chinese - need to be considered. An insistence that ‘there is a pandemic’ may be stated for reasons other than disease prevention. Similarly, the potential profit motives for ‘discoveries’ by pharmaceutical businesses must be considered when new drugs or treatments become available; there may not actually be a condition that needs to be treated. (The mass prescription of statins for cholesterol issues over recent years may, perhaps, turn out to have been of little benefit to patients.)
Doctors and other specialists should be encouraged to keep abreast of the latest research, independently of pharmaceutical or political organisations; indeed there is a case for discouraging - or even banning - those establishments involved in the education of doctors from taking sponsorship from political or pharmaceutical businesses because of the possible conflicts of interest.
This may affect all aspects of the NHS.
It could be implemented in a couple of years but will probably take much longer.
6. More focus on alternatives to medication, immunisation and surgery - nutrition, exercise, lifestyle
At present the initial response of any practitioner to learning of a medical issue seems to be to suggest medication, rather than to determine what the actual cause of the condition might be. This response may stem from there being much training material provided by pharmaceutical companies.
Other options should be explored first. Lifestyle and exercise, and especially, nutrition. The importance of vitamin D is ignored within ‘our NHS’, despite there being a recommendation on the NHS website that all adults should take a vitamin D supplement in the winter. Indeed, I know of a cancer patient on immunotherapy who asked her doctor about the relevance of any supplements to her treatment, and was specifically told that she did not need to take any supplements - going against the apparent NHS recommendation for vitamin D.
The immune systems of long-term patients in hospitals would surely benefit from a daily vitamin D supplement.
This change would mostly affect hospitals and GPs, but potentially all parts of the NHS.
This change could be implemented quite quickly, just requiring some training for practitioners.
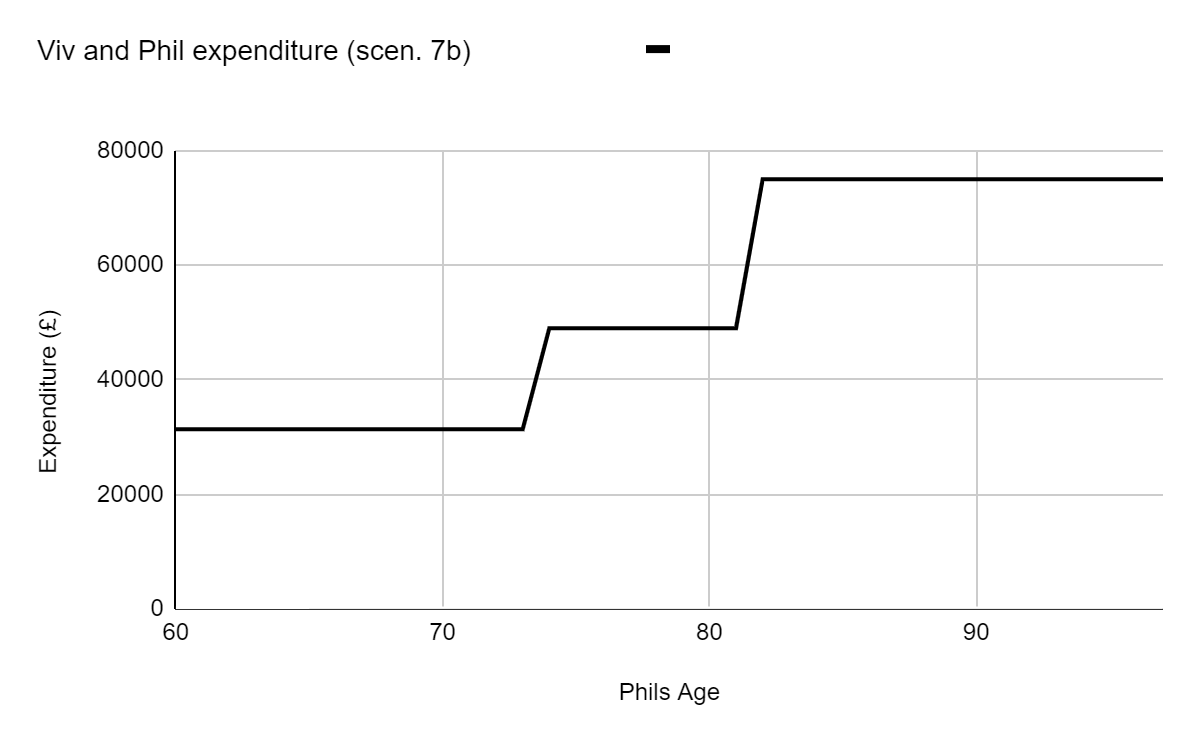
7. The public should pay towards NHS services through some form of insurance
There is a strong argument that the government should introduce some form of insurance scheme to control access to the NHS; everyone would pay a small premium, and be required to provide proof of this insurance when they benefit from NHS treatment. This could be managed by the government and, of necessity, be heavily subsidised - but it could bring in additional funds, and would enable each patient’s risk to be assessed and the premium adjusted accordingly.
Someone who has no insurance would only be entitled to essential life-saving treatment free of charge.
Key data - such as weight, height (or BMI), age, etc should be included on the Summary Care Record and used as a basis for insurance premiums. (The provision of annual statements to patients would allow patients an opportunity to check and challenge this information).
This may affect all aspects of the NHS.
It could be implemented in a couple of years but will probably take much longer.
8. Require doctor and other specialist training costs to be repaid if they work outside NHS
A significant problem seems to be that doctors, and other specialists, are often trained at NHS expense, and then go to work elsewhere because the salaries are higher (although local doctors may have to pay back loans covering the cost of their training.)
A scheme should be implemented whereby those graduating after studying medicine are deemed to have been leant the funds to do this by the NHS, and (in effect) repay this loan over a number of years by working in the NHS. Those that don’t keep up the repayments are required to repay the loan from their earnings elsewhere.
Guarantors living in the UK could be sought for the loan - perhaps parents - to ensure that the costs could be recovered in the event of the beneficiary working overseas.
This would affect principally hospitals and GP surgeries.
It could be implemented in a couple of years but will probably take much longer.
9. Restore junior doctor experience to levels of the past
Prior to 2004 junior doctors often worked shifts of up to 120 hours a week.
While stressful, this provided them with a level of experience that more recent trainees have lacked. Doctor experience should be likened to that of a pilot - whose flying hours are a measure of their experience; reducing junior doctor working hours from 120 to 48 per week has resulted in young doctors often having insufficient experience to handle complex situations.
The amount of time doctors spend in junior roles (and on commensurate salaries) should be revised upwards to they gain necessary experience to progress to more senior roles.
This would affect hospitals.
It could be implemented in a couple of years but will probably take much longer; there will probably be much opposition from the BMA.
10. Work with Government Departments and other agencies to encourage environments likely to facilitate mobility and good health
The NHS, or an associated agency, should work with national and local government departments and agencies to ensure that health impacts of key governmental decisions are all positive. For example, input could be given to departments as follows:
Transport - regarding the value of encouraging walking, having clear and level pavements, and good footpath networks; also regarding the value of public transport (users of which may tend to be healthier than people who drive everywhere)
Environment - regarding street design, layout and location of new developments, to encourage non-car transport
Employment / Industry - regarding working from home; encouraging work styles that involve regular movement, personal interaction with others, leaving the desk, etc.
This relates to keeping people healthy.
It could be started within a couple of years but would be an ongoing task.
11. Change audiology services to work like ophthalmology
At present audiology services (at least in the BLMKICB area) are something of a shambles; anyone with hearing issues is directed to their local branch of Specsavers, who perform a rudimentary test, and then try to sell them an expensive hearing aid. (A ‘free’ NHS one is an option, but, if chosen, is hastily configured and may well not work well for the patient; also, no follow up is undertaken.)
Audiology should operate like ophthalmology: patients should be able to get an NHS hearing test at any audiologists, and NHS funding should be used to either buy a basic hearing aid, or to subsidise or more elaborate one. Follow up checks should be provided by the NHS. All rather like getting your eyes tested at the opticians.
Further, ear wax removal should be available on the NHS.
These changes would affect audiology services.
They could be implemented in perhaps 2 years but will probably take longer because of vested interests.
12. Long term use of medication should be monitored
One of the many limitations of the Summary Care Record at present is that it does not say how long a patient has been on the medication that they are prescribed; it lists the medication a patient is prescribed, but not the start date for each.
Long term use of many medications can cause problems, and needs to be ruled out as the cause of an issue when a patient presents at their GP or hospital.
My own father was severely ill in 1994 having been on blood pressure medication for 16 years that he should not have taken for more than two; I myself was on PPIs (omeprazole) for five years without any checks from GPs or anyone despite checks of magnesium and vitamin B12 levels apparently being recommended for anyone on such medication for more than two years.
If the start date is accurately recorded in the SCR a simple computer program can be run for the GP to identify patients who need to be checked; also, information would be available for anyone presenting at A&E with symptoms possibly caused by long term medication use.
This would affect IT systems, GPs and hospitals - principally A&E departments.
This change could be implemented in under 2 years, initial setup of the data might be challenging unless the patient is involved.
13. Spare capacity needs to be built into the system
Since the 1960s it has been fashionable among business leaders to avoid having spare (i.e., unused for much of the time) capacity in any system. Dr. Beeching removed it from the railways; now, additional rail capacity is needed, and it is very challenging adding it.
This problem has arisen in hospitals; the number of beds available in the NHS has reduced greatly in recent years. It was not felt acceptable to have spare capacity in the system.
Unfortunately, as the population has grown, and aged, there is more demand than there used to be. As with the railways, it is a devil of a job to add in capacity, and, as a result, patients wait in corridors, and outside A&E in ambulances, using up an ambulance resource that should be out helping another patient. Indeed, I have sat with a patient in an ambulance for several hours, for the crew it was the only patient they helped that day.
It is not just a case of buildings; for instance staffing structures need to be more flexible, so that, when necessary, additional nursing resources can be deployed. In the past there were military hospitals, and first aiders, who could be deployed to help civilians if needed; the military have been so run down that this option is probably no longer available. Possibly, there might be a case to encourage many in the community to train as ‘territorial’ hospital staff, rather like Army territorials, who could be called upon to help at time of need.
Those trained in such a way would not only be able to help when required but also be well equipped to support family and friends who might need care in the future.
This would affect hospitals.
This could be introduced in a couple of years but will probably face much union opposition.
Comments
Post a Comment